Malarial plasmodium in the human body - infection, symptoms and treatment
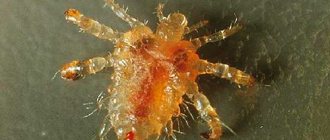
So, Plasmodium falciparum is the causative agent of malaria infection. According to the classification of protozoan (unicellular) parasites, it belongs to the phylum Apicomplexa, class Sporozoa, family Plasmodiidae, genus Plasmodium. And the English scientist Donald Ross discovered and experimentally proved the presence of a parasitic protozoan - malarial plasmodium in the saliva and intestines of a female mosquito of the genus Anopheles.
There are 4 types of parasites that can parasitize the human body:
- Plasmodium vivax is the causative agent of tertian malaria;
- Plasmodium malariae is the causative agent of four-day malaria;
- Plasmodium falciparum is the causative agent of tropical malaria;
- Plasmodium ovale is the causative agent of ovale malaria, similar to the species P. vivax.
All varieties are generally similar in shape, structure and life cycles. An interesting feature of parasites of the Apicomplexa type is the ability to alternate sexual (gamogony) and asexual (agamogony) methods of reproduction in the life cycle. In this case, a change of “master” occurs. In the human body, which is an “intermediate host” for the malarial plasmodium, only asexual reproduction is possible. And the phase of sexual reproduction is the prerogative of the main “host” and carrier of malaria, that is, the mosquito.
The female malaria mosquito is only a carrier of infection. When a person is bitten, the saliva of an infected mosquito enters the bloodstream, and sporozoites come with it. Symptoms of infection that manifest themselves in the disease are characteristic only of humans. Thus, the etiology of human malaria is infection when sporozoites of malarial plasmodium enter the blood.
Infection is possible in several ways:
- when bitten by a female Anopheles mosquito;
- during blood transfusion (hemotransfusion);
- for injections (through medical instruments);
- transplacental route (from a sick mother in labor to a child).
Periods and symptoms of the disease
The entire process, from infection to recovery, can be divided into four periods: incubation, acute, latent and relapse. The nature of the course of the disease and the frequency of relapses largely depend on the type of malarial plasmodium - the causative agent. For example, the incubation period of the disease can vary from 7 days to 1 year, depending on the type of malaria infection.
General characteristic signs of the disease:
- elevated body temperature (39 – 40 degrees); chills and fever replace each other;
- “ache” throughout the body;
- prolonged headaches;
- gagging and diarrhea;
- profuse sweating after a hot flash;
- severe enlargement of the liver and spleen;
- pain in the liver area;
- general weakness and anemia;
- possible confusion;
- yellowing of the skin and sclera of the eyes;
- frequent and painful urination;
- loss of appetite;
- insomnia.
Individual signs and symptoms (for example: cardiac stabbing pain, asthma attacks, joint pain) are also possible and depend on the presence of “weak points” in the body and the functioning of the immune system. Sick children usually develop a rash on their body. Tremors of the limbs are also typical for infants.
The initial symptoms of malaria can easily be mistaken for ARVI. But a very clear frequency of repetition of an attack of the disease (alternating chills and fever, ending with profuse sweating) is a distinctive feature of malaria and should be a signal to contact the clinic for advice. Especially if the patient has recently traveled and vacationed in countries with a hot tropical climate.
Diagnostics
In addition to the clinical assessment of the patient’s condition (based on the symptoms of the disease), laboratory methods for diagnosing malaria are used in medical practice. Malarial plasmodium manifests itself in blood tests at all stages of the disease before the onset of treatment. Therefore, special tests can determine its presence in the blood.
- The “thick drop of blood” method (Allows, at a minimum, to detect the presence of infection);
- Thin blood smear (Used to determine the type of malarial plasmodium - the pathogen and the stage of its development. This is necessary for the subsequent selection and prescription of drug treatment);
- Serological method (Detects the presence of antibodies to malaria in venous blood. A positive test result may also indicate a previous disease);
- PCR method - polymerase chain reaction (Used as an additional research method, along with the “thick drop” analysis, to detect malarial plasmodium at low concentrations in the blood).
In addition to specific diagnostic methods, the presence of infection is manifested in the form of deviations from the norm in a general blood test (hypochromic anemia, leukocytosis, thrombocytopenia). A general urine test also detects pathology based on indirect signs: hemoglobinuria and hematuria.
Traditional treatment
In medical practice, for the treatment of malaria, etiotropic therapy is used, aimed at localizing and combating the causative agent of the disease. For its effectiveness, preliminary laboratory diagnosis and correct selection of drugs are important. Depending on the type of malarial plasmodium and the stage of the disease, the patient may be prescribed various antimalarial drugs, as well as a combination of drugs.
Traditional medicine in the fight against malaria
Folk remedies for the treatment of malaria can be divided into basic and auxiliary, aimed at restoring the functioning of organs, detoxifying the body and increasing immunity.
Cinchona
The main and most effective means include treatment with cinchona bark powder. Here are two recipes for using this product:
- Take half a gram of quinine powder for five days exactly at sunrise. Then take a break for two days, and then resume taking the powder for another two days. An important condition is the need to sleep after taking the medicine.
- Prepare a fabric bag with quinine powder (10 grams of powder per bag) and place it on the patient’s chest for 3 to 4 hours. The medicine is absorbed by the body directly through the pores of the skin, which promotes rapid healing.
willow bark
Another effective treatment for malaria is the bark of willow branches. To prepare the medicine, you need to take a handful of bark and boil it in about three hundred ml of water until the volume of the liquid is reduced by one and a half times (to one glass). Take on an empty stomach for several days until the condition significantly improves. In addition to this recipe, it is also recommended to generously cover the patient’s bed with willow leaves during attacks, covering the top with a thin cloth.
Lilac and sunflower
Lilac leaves and sunflower inflorescences are also popular medicine remedies for malaria. An infusion of 20 lilac leaves in a glass of boiling water, kept warm for 1.5 hours, is taken twice a day, in the morning on an empty stomach and in the evening before bed, for 10 days.
Cut off the sunflower inflorescence when its petals begin to fall, chop it finely into a bottle and fill it with vodka. Cover the bottle with gauze, keep in a sunny place and leave for a month. Take 20 drops before the next attack or three times a day before meals.
Chicory and licorice
Good auxiliaries for quickly cleansing the lymphatic system and restoring the immune system are chicory root and licorice root.
Pour 10 grams of crushed licorice root into a container and add 200 ml of water. Keep in a water bath for half an hour. Cool the broth, strain and bring boiling water to 200 ml. You can drink the resulting decoction up to 5 times a day, at least an hour before meals. Portion for one serving – 5 tablespoons.
Preparation of chicory root decoction: pour 1 tablespoon of chicory root into 0.5 liters of water, bring to a boil and simmer for 20 minutes. Cool, strain and take 1 tablespoon three times a day before meals.
Garlic
Garlic is used as a natural antibiotic in the treatment of malaria. Preparation: Chop 2 peeled and washed heads of garlic and add a glass of cool, clean water. Leave for 12 hours. Take several sips during attacks while lying in bed. Approximately 1 glass per day for five days.
Prevention
Traditional medicine today cannot offer an effective vaccine against malaria. But research towards the development of such a vaccine is actively underway. To select a drug, it is important to know the type of pathogen that can be encountered in a given area, its resistance to the listed drugs, as well as possible side effects from taking the listed drugs. Any of the drugs must be taken at least a week before traveling to a disadvantaged region and continued for another month after leaving the danger zone.
Using mosquito nets, repellents (to repel mosquitoes), and mosquito killers reduces the risk of insect bites and infection.
At home, folk remedies are also used: peppermint, thyme, rosemary, geranium, basil, wormwood, lemon balm, cloves and eucalyptus. The smell of these plants repels dangerous insects.
Rapid and timely identification of malaria patients, their hospitalization and treatment are also measures to prevent the epidemic.
Instructor-valeologist Natalya Dudarchik
Story
It is believed that people have been suffering from malaria for 50,000 years. Malaria is believed to be native to West Africa (P. falciparum) and Central Africa (P. vivax). Molecular genetic evidence suggests that the preparasitic ancestor of Plasmodium was a free-living protozoan capable of photosynthesis that adapted to live in the intestines of aquatic invertebrates. It could also live in the larvae of the first blood-sucking insects of the order Diptera, which appeared 150-200 million years ago, quickly acquiring the ability to have two hosts. With the advent of humans, malaria parasites evolved that were capable of changing hosts between humans and mosquitoes of the genus Anopheles. The oldest mosquito fossils found containing remains of malaria parasites are 30 million years old.
The first chronicled evidence of fever caused by malaria was discovered in China. They date back to approximately 2700 BC. e., during the reign of the Xia dynasty.
Types (forms) of malaria
The symptoms, course and prognosis of the disease partly depend on the type of plasmodium, which is the causative agent of this form of the disease.
The causative agent of tropical malaria is P. falciparum. Causes the most dangerous form, often accompanied by complications and a high mortality rate. This form is the most widespread (91% of all malaria cases in 2006).
The causative agent of four-day malaria is Plasmodium malariae. Attacks usually occur within 72 hours.
The causative agents of three-day malaria and the similar oval malaria are Plasmodium vivax and Plasmodium ovale, respectively. Attacks occur every 40-48 hours.
These forms of malaria also differ in the length of the incubation period, the duration of different stages of the life cycle of plasmodium, symptoms and course.
Destruction of mosquitoes
Efforts to control malaria by killing mosquitoes have achieved success in some areas. Malaria was once common in the United States and Southern Europe, but the draining of swamps and improved sanitation, along with the control and treatment of infected people, have removed these areas from being unsafe. For example, in 2002, there were 1,059 cases of malaria in the United States, including 8 deaths. On the other hand, malaria has not been eradicated in many parts of the world, especially in developing countries - the problem is most widespread in Africa.
DDT has proven itself to be an effective chemical against mosquitoes. It was developed during World War II as the first modern insecticide. It was first used to fight malaria and then spread to agriculture. Over time, pest control, rather than mosquito eradication, has come to dominate the use of DDT, especially in developing countries. Throughout the 1960s, evidence of the negative effects of its misuse increased, eventually leading to the ban of DDT in many countries in the 1970s. Prior to this time, its widespread use had already led to the emergence of DDT-resistant mosquito populations in many areas. But now there is the prospect of a possible return of DDT. The World Health Organization (WHO) now recommends the use of DDT against malaria in endemic areas. In addition, the use of alternative insecticides in areas where mosquitoes are resistant to DDT is proposed to control the evolution of resistance.
Vaccines
In November 2012, findings from a phase III trial of an experimental malaria vaccine known as RTS, S reported that it provides modest protection against clinical and severe malaria in young children. Efficacy was in infants from 6 to 12 weeks of age and about 50% in infants from 5 to 17 months of age in the first year of the trial.
The RTS,S vaccine was developed using a fusion of hepatitis B surface proteins containing epitopes of the Plasmodium falciparum
malaria sporozite, which grows in yeast cells. It also contains a chemical adjuvant to boost the immune system. The vaccine is being developed by PATH and GlaxoSmithKline (GSK), which spent about $300 million on the project, plus about $200 million more from Bill and Melinda Gates.
Mosquito nets and repellents
Mosquito net is an effective measure against malaria
Mosquito nets help keep mosquitoes away from people and thereby significantly reduce the number of infections and transmission of malaria. Nets are not a perfect barrier, so they are often used in conjunction with an insecticide that is sprayed to kill mosquitoes before they find their way through the net. Therefore, insecticide-impregnated nets are much more effective.
Covered clothing and repellents are also effective for personal protection. Repellents fall into two categories: natural and synthetic. Common natural repellents are essential oils of certain plants.
Examples of synthetic repellents:
DEET (active ingredient - diethyltoluamide) (eng. DEET, N,N-diethyl-m-toluamine)
Folk remedies
Medicines are the mainstay of malaria treatment.
But many sources indicate the benefits of some natural remedies in the treatment of disease caused by Plasmodium. Here we publish only a few of them, and in no case should these recipes and recommendations be considered as the main means of treatment. Lime and lemon are beneficial for four day fever. About three grams of chalk are dissolved in 60 ml of water and the juice of one lemon or lime is added. This composition must be drunk before the onset of fever.
Alum is also considered as a supportive agent in the treatment of malaria. They are fried in a hot frying pan and ground into powder. Take a teaspoon of the drug internally four hours before the expected fever and half a teaspoon two hours after it.
Finding out the cause of the disease
In 1880, French military doctor Charles Louis Alphonse Laveran, working in Algeria, suggested that malaria was caused by protozoa. This was the first time that protozoa were identified as the cause of disease. For this and other discoveries he was awarded the Nobel Prize in Physiology or Medicine in 1907. The genus name of the parasite Plasmodium was proposed in 1895 by Italian scientists Ettore Marchiafava and Angelo Celli. A year later, Cuban doctor Carlos Finlay, who was treating yellow fever patients in Havana, first suggested that the disease could be transmitted to humans by mosquitoes. The Englishman Sir Ronald Ross, working in India, showed in 1898 that certain species of mosquitoes transmit malaria to birds, and isolated parasites from the salivary glands of the mosquito. He also managed to find parasites in the intestines of mosquitoes that fed on the blood of sick people, but was unable to trace the transmission of parasites from mosquitoes to humans. In 1898, Giovanni Batista Grassi managed to experimentally infect a person with malaria through a mosquito bite (he experimented on volunteers, including himself). He also proved that only mosquitoes of the genus Anopheles are carriers of malaria in Italy, and developed and implemented measures for the prevention of malaria. However, in 1902, only Ronald Ross received the Nobel Prize in Medicine for describing the life cycle of the malaria parasite. The data obtained by Finlay and Ross were confirmed in 1900 by the medical council, headed by Walter Reed. The recommendations of this council were used by William C. Gordas for the health measures carried out during the construction of the Panama Canal.
Doxycycline
Doxycycline is a broad-spectrum tetracycline drug. The doctor prescribes doxycycline for infections caused by pathogenic microorganisms.
Doxycycline ointment has good and effective results, which helps not only as a treatment, but also as a prophylactic agent. The ointment is applied to the skin areas where insect bites were found.
Primaquin
Primaquine is a drug that stops the proliferation of the malaria pathogen. Can be used for any type of disease development. A good prophylactic, reduces the risk of relapse. In case of overdose or prolonged use, the following adverse reactions from the body may develop:
- Migraine.
- Abdominal pain.
- Pathologies of the cardiovascular system.
- Cyanosis of lips.
- Anemia.
Bigumal
Bigumal is an antimalarial drug that destroys the causative agent of the disease and relieves inflammation in the body. Suitable not only for the treatment of malarial pathology, but also as a preventive measure.
Bigumal is prescribed for intrauterine infection, but the dosage is prescribed by the doctor. If used incorrectly, the following symptoms may develop:
- Nausea and vomiting.
- Cyanosis of lips.
- Sudden changes in temperature.
Cannot be used if therapy with other means has already begun. It is also worth refusing to take pills for patients with kidney or vascular dysfunction.
Mefloquine
Mefloquine is a man-made malaria drug that targets the malaria pathogen. However, there is a big drawback: the pathogen quickly gets used to the drug and mefloquine has no effect on it.
If the patient does not have the opportunity to quickly go to a clinic to make a diagnosis and begin treatment, doctors recommend starting to use mefloquine on their own. If the patient has an individual intolerance to the components, you should stop taking the pills.
All drugs for the treatment of malaria are selected by the doctor on an individual basis.
Antimalarial immunity
The immune response against malaria infection develops slowly. It is characterized by low efficiency and practically does not protect against re-infection. Acquired immunity develops after several malaria infections over several years. This immunity is specific to the stage of the disease, to the species, and even to a specific strain of Plasmodium falciparum. But clinical manifestations and symptoms decrease with the development of specific antimalarial immunity.
Possible explanations for this weak immune response include the presence of Plasmodium falciparum in cells during most of its life cycle, general suppression of the immune system, the presence of antigens that are not recognized by T cells, suppression of B cell proliferation, significant polymorphism of Plasmodium falciparum and rapid change of potential antigens on its surface.